Thaw - My Dream Project

Project Name
Thaw
Headquarters
Houten
Industry
Healthcare
Company Size
1
Timeline
3+ Months
Understand
Thaw is rooted in personal experience with trauma-related freeze responses; moments when initiation becomes nearly impossible and even simple actions feel disproportionately hard.
Freeze is not a lack of willpower. It is a physiological response in which the nervous system enters a state of dorsal vagal activation. Freeze does not remove agency, but suppresses initiation and drastically raises the threshold for action. This makes it uniquely difficult to design for: the state is invisible, differs per individual, and the user has the least capacity to actively do anything at exactly the moment it matters the most. This is precisely what shaped the design direction of Thaw: not a system that acts on behalf of the user, but one that lowers the threshold just enough for the user to act themselves. The goal is not to take over, but to make initiation accessible again.
What makes this design challenge particularly complex is that freeze is physiologically similar to several benign states, for example sitting still during a film, resting, sleeping. Without personal calibration, a detection system would produce far too many false positives.
A review of wearable health landscape suggests that trauma-informed design principles are rarely applied explicitly, particularly in the context of freeze or dorsal vagal states. The existing products in this space, including Apollo Neuro, Fitbit and Empatica, do not address this combination. That gap is where Thaw begins.
Observe
What research tells us about freeze
Freeze has a measurable physiological signature. This follows from research into the autonomic nervous system, including the work of Stephen Porges (1995, 2003), who described through Polyvagal Theory how the nervous system responds to threat via a hierarchy of reactions, from social engagement to fight/flight, to freeze. Importantly, several core claims of polyvagal Theory remain scientifically contested (Grossman & Taylor, 2007; Barnett et al, 2023). The broader finding, that freeze has a recognisable physiological pattern, is, however, widely supported in autonomic neuroscience and trauma literature.
Four signals are measurable via wearable sensors:
Immobility: sustained stillness is the simplest and most direct signal, measurable via an accelerometer.
Heart rate variability (HRV): the variation in time between heartbeats reflects autonomic nervous system activity. In freeze, the pattern is not simply low, but abnormally rigid. Variability nearly disappears while heart rate simultaneously slows, typically preceded by a brief acceleration.
Electrodermal activity (EDA): under stress, the skin conducts slightly more electricity. In freeze, conductance drops instead, as the sympathetic nervous system withdraws. This distinguishes freeze from fight/flight.
Skin temperature: during freeze, blood vessels constrict, causing measurable temperature drop at the extremities.
What research tells us about intervention
For the intervention, haptic feedback (i.e. subtle vibrations on the skin) has the strongest evidence base. Research shows that vibrations delivered at a frequency lower than the heartbeat have a calming effect by offering the body a sensory anchor the nervous system can entrain to, without requiring the user to actively do anything (Azevedo et al, 2017; Costa et al, 2019). The mechanism is significant: haptic stimuli bypass cognitive processing and reach the body directly, making them particularly suited for states in which cognitive initiation is precisely what is impaired.
The combination of these signals within a single system, as Thaw proposes, has not previously been studied specifically in freeze states. That is exactly the gap this project addresses.
Define
Research question:
"How can we design a wearable system that, based on personalized patterns of immobility and physiological signals, detect a freeze-like state, and through subtle tactile cues lowers the threshold for initiation, without adding extra pressure, shame or performance expectations?"
The design problem has two layers: detection (recognizing when someone in in freeze) and activation (lowering the threshold for action without adding cognitive load). The core of trauma-informed design here is that the user always retains full agency. The system supports and signals, it does not instruct or steer. It is a noticing tool, not an intervention device
A key insight that shapes this design direction is that freeze is often invisible to the person experiencing it. Research shows that the freeze response is characterized by immobilization, numbing and dissociation. These are neurologically driven reactions that reduce access to reflective awareness (Lanius et al., 2025). Brain regions associated with interoceptive awareness, the ability to perceive one's own bodily signals, show reduced activation in individuals with trauma histories, impairing the ability to recognize and interpret physical sensations (Baxter et al., 2024). As Van der Kolk (2014) notes: when someone is frozen, the prefrontal cortex is offline, nothing can come in until the freeze is interrupted.
This is precisely why Thaw operates through the body rather than the mind. The device detects what the person cannot perceive themselves, and responds through a sensory channel that bypasses the cognitive block. It does not require action. It simply arrives, earlier than awareness does.
Timing matters
This timing matters. The earlier a freeze state is detected, the lower the threshold for action still is. The longer freeze goes unnoticed, the harder it becomes to initiate anything at all. Thaw is designed to intervene at the earliest measurable moment and not when the person has already been stuck for an hour, but at a point where the smallest nudge may still be enough.
Thaw closes the loop between detection and intervention, specifically for freeze states, with trauma-informed design principles. No existing product does this. Three design principles guide every decision:
Restoring agency, not control. The user can always immediately stop, confirm or ignore. The button is available, never obligatory.
Non-response is a valid response. The device never escalates. After a maximum of three attempts it withdraws and stops completely.
Personal calibration is essential. A generic model produces too many false positives. The system learns your freeze signature versus your normal stillness.
Ideate
Three evidence-based haptic patterns form the core of the intervention. They bypass the initiation barrier: they ask nothing of the user, but offer a sensory anchor the nervous system can entrain to.
Tidal Breath: Sinusoidal: 5s build-up / 5s fade, starting barely perceptible (30–40%). Based on 6 breaths per minute for cardiac coherence.
Heartbeat Anchor: Lub-dub pulse pattern at 20% below personal resting heart rate. Based on Doppel research showing reduced anxiety and skin conductance.
Grounding Tap: Irregular gentle taps at 3–5s intervals. Prevents habituation and stimulates body awareness.
Pattern selection logic
Thaw follows a fixed sequence ordered by gentleness: Tidal Breath first, Heartbeat Anchor second, Grounding Tap third. From barely perceptible to more body-directed. Never the other way around. Over time, the system can learn which pattern tends to work best for this specific user, based on what preceded moments of movement. Personal response history may eventually replace the fixed default.
What remains constant: the device never increases intensity, never skips ahead, and never exceeds three attempts. The ceiling is fixed. Only the starting point may vary. The escalation logic inverts conventional UX logic: de-escalate, never escalate. Patterns become softer, not louder. The device never asks "are you okay?" because that would recreate a power imbalance. Anti-patterns are defined just as consciously as the patterns themselves:
No punitive feedback: no "you froze again" messages, no episode-counting as failure.
No surveillance: local processing, user initiates data review themselves.
No paternalism: offers sensation, not instruction. Never "try to breathe".
No coercion: hard limit of 3 attempts, then complete silence.
Technical Architecture
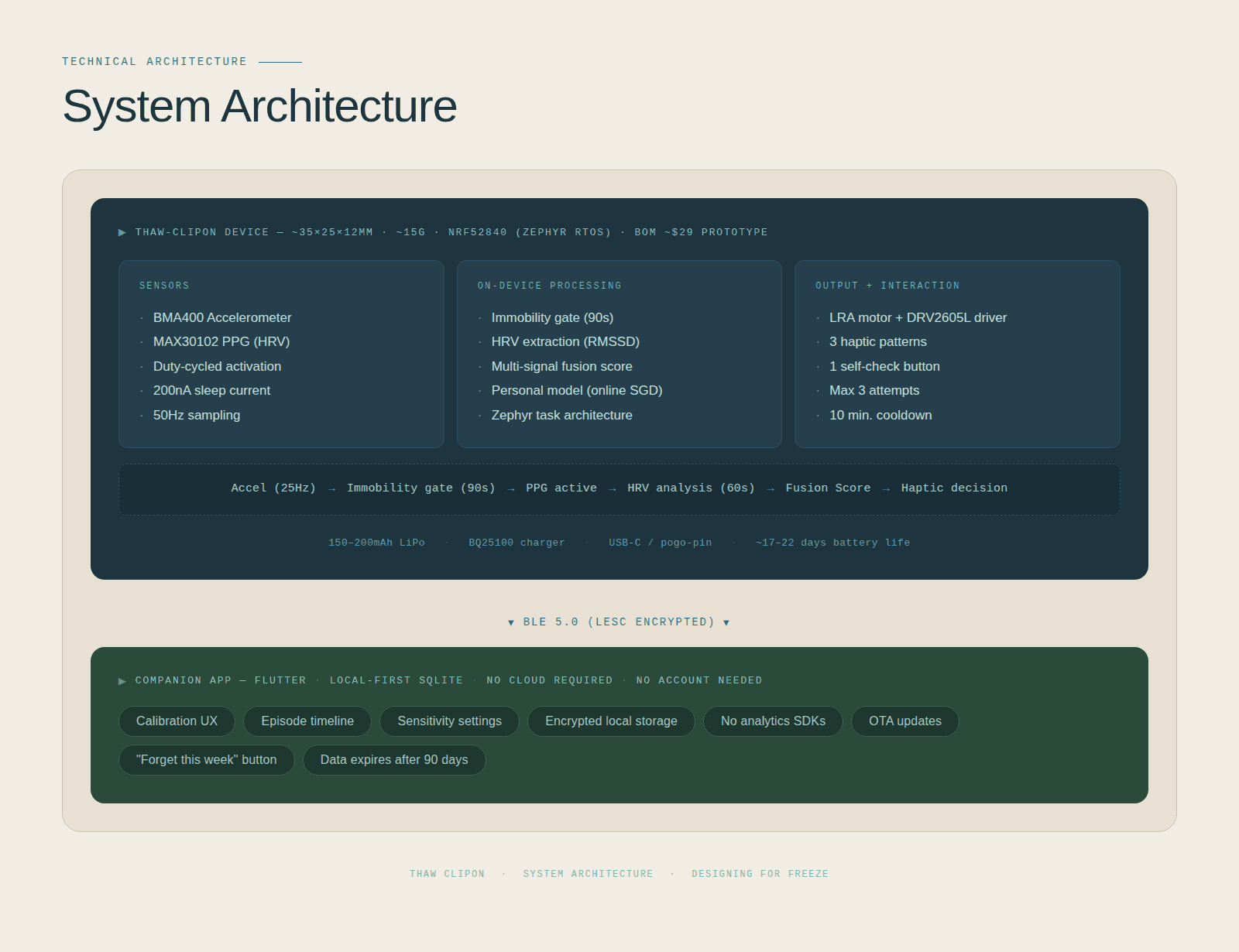
System Architecture: designed with Claude Code
The Thaw-ClipOn is a small clip-on device. It is roughly the size of a large paperclip, weighing just 15 grams. It runs on the nRF52840, a compact low-power chip commonly used in wearable technology, paired with Zephyr RTOS: a lightweight operating system that allows the device to handle multiple tasks simultaneously, such as sensing and communicating. The estimated cost of all components for a single prototype is approximately $29.
The device uses two sensors:
The first is an accelerometer, the same type of sensor that detects movement in a smartphone, which measures whether the user has been still for an extended period.
The second is a PPG sensor, which shines a small light onto the skin and measures blood flow to derive heart rate and HRV. This is the same technology used in most smartwatches today.
Detection follows a fixed pipeline. First, the accelerometer checks for sustained stillness: an immobility gate that prevents unnecessary activation. If stillness is detected, the PPG sensor switches on to measure HRV. These two signals are combined into a single fusion score, which determines whether a haptic cue is triggered. Everything is processed locally on the device itself. Nothing is sent to a server or the cloud. Battery life is estimated at 17–22 days on a single charge.
The companion app is built in Flutter, which allows it to run on both iPhone and Android from a single codebase. All data is stored locally on the user's phone using SQLite, a small, lightweight database that requires no account and no internet connection. There are no third-party analytics, no data sharing, and a "Forget this week" button that permanently deletes all recent data. Everything expires automatically after 90 days.
Prototype
Form factor: what shape does Thaw take?
Three forms were explored: a ring, a clip-on, and a handheld stone. The stone was ruled out first, because it only measures when actively held. And that is precisely the problem: in freeze, that kind of initiation is out of reach.
Reliable detection requires continuous, passive skin contact without the user having to do anything. That means a wearable. The clip-on is the chosen form for the first prototype: practical, discreet, and suited for consistent sensing. The ring is an interesting future direction, but requires further miniaturisation.
What can the first prototype already do?
The first prototype is intentionally simple: detect stillness, deliver a haptic cue, and offer one button. No heart rate sensor yet, no skin conductance, that comes later. First, the core interaction needs to work and be tested.
The first 48 hours, the device does nothing but learn. No cues yet but observation only. The word 'trauma' is avoided in the app unless the user introduces it. Instead: 'pause state' and 'getting stuck'.
Build phases:
Phase 1 : First working prototype: sensing, Bluetooth, button triggers vibration
Phase 2 : Firmware: signal processing, power optimisation
Phase 3: App: device connection, calibration flow, trauma-informed UX
Phase 4: Integration: OTA updates, custom PCB, user testing
Test
Testing with people who have experienced trauma requires careful ethical frameworks. In the Netherlands, this will likely require approval from a medical ethics committee (METC).
Detection starts deliberately conservative. The device activates too little rather than too much. A device that rarely triggers but is right when it does builds trust.
We start with non-clinical populations, measure adverse effects, and check in on consent throughout. Every test session is followed by a debrief.
Four risks are actively managed:
Too many activations: annoying, or potentially unwanted. Solution: conservative defaults and a one-week learning period.
Too few activations: if the device never responds, the user loses trust. Solution: graduated response based on confidence score.
Dependency: the risk that people become less able to sense their own body. Solution: Thaw is a temporary support tool, not a permanent solution.
Hypervigilance: being constantly monitored can increase anxiety. Solution: minimal data visible, user decides when to view it.
Trauma-informed design, rigorously applied to wearable technology, remains largely unexplored. That is where the potential for an original academic contribution lies.
A full literature list is available upon request

